Neuromuscular blocking agents- (Act on NM junction)
|
|
Depolarizing / Non-competitive (Mnemonic: DNS) |
Non-Depolarizing / Competitive blockers |
|
Example |
Only one drug Succinyl choline / Suxamethonium |
Rest all NM blockers |
|
Fasciculation |
Seen |
Not seen |
|
Post OP myalgia |
Present |
Absent |
|
Reversal by Neostigmine |
No |
Yes |
|
Train of four response |
Absent |
Present |
|
Train of four ratio |
1 |
<1 |
|
Post tetanic fecilitation |
Not seen |
• May be present • Absent- If block is profound |
Succinyl choline / Suxamethonium-
• Di choline ester (2 molecules of ester)
• MOA: Persist depolarization of muscle end plate
S/E-
• It can trigger malignant hyperthermia (Only in pt with defective gene)
• Hyperkalemia (so not given in Burn, Trauma, Paraplegia, Muscular dystrophy, Muscle atrophy)
• Fasciculation
• Increases - Intra cranial pressure, Intra ocular pressure, Intra gastric pressure
Polarizing / Competitive blockers-
|
Benzyl iso quinoline |
|
Amino steroid |
|
• D-tubocurare • Doxa curium |
Long acting |
• Pan curonium • Pipe curonium |
|
• Atra curium • Cis-Atra curium
both inactivated by “Hofman’s elimination” (Spontaneous non-enzymatic so use in liver & kidney |
Intermediate Acting |
• Ve curonium • Ro curonium
both not use in liver & kidney disease. |
|
Miva curium
It’s metabolise by “Pseudo choline esterase” |
Short Acting |
Rapa curium |
|
Yes |
Histamine Release |
No
(Amino = No) |
|
Present |
Histamine- • It’s vasodialator • BP decrease • HR increase • Bronchospasm • Flushing |
Absent |
|
No (Due to tachycardia it’s CVS unsatble) |
CVS stable |
Yes |
Note- ‘Laudanosine’ is the metabolite of atracurium and it’s responsible for seizure.
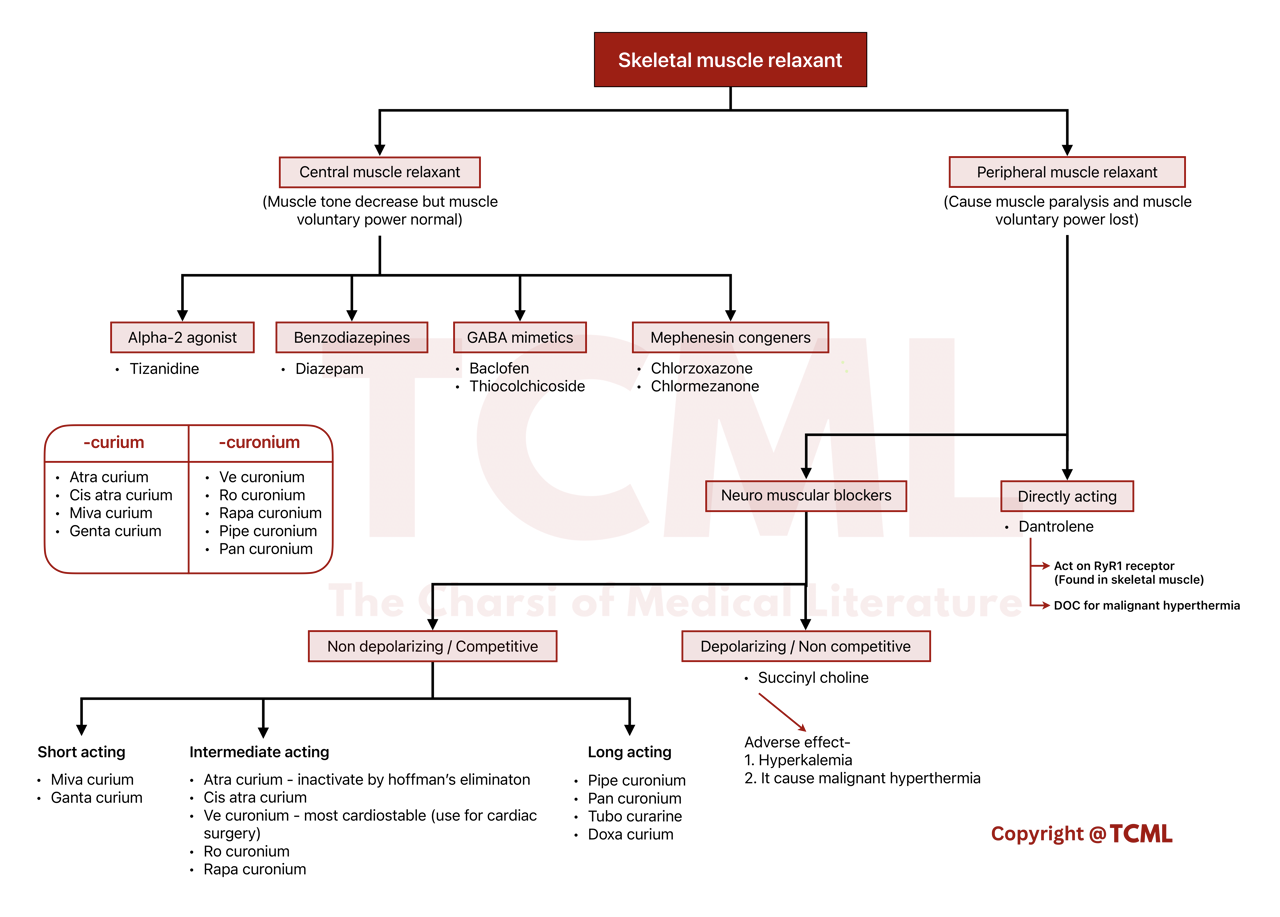
 Figure- Baclofen (Central muscle relaxant)
Figure- Baclofen (Central muscle relaxant)
 Figure- Thiocolchicoside (Central muscle relaxant)
Figure- Thiocolchicoside (Central muscle relaxant)